
Understanding Diabetes
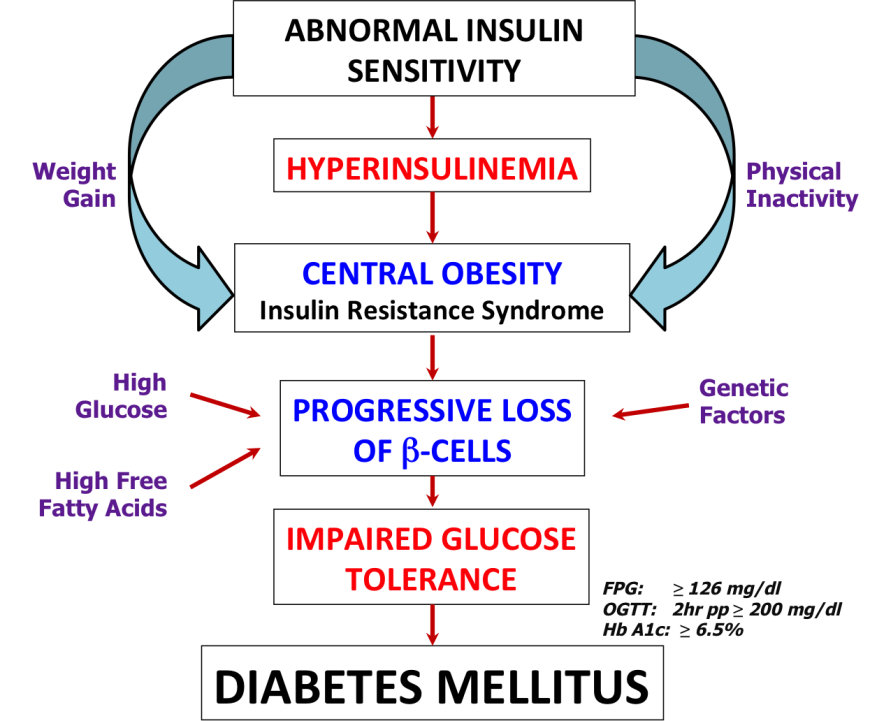
Diabetes Mellitus (DM) is a group of chronic progressive metabolic diseases with increasing worldwide prevalence. It is commonly characterized by hyperglycemia - meaning high levels of glucose in the blood. The primary cause of diabetes is the absence of a hormone called insulin (Figure 1) and/or the inability of muscle and fat cells in the body to respond to this hormone and use glucose.
What's in a Name?
The term “Diabetes Mellitus” is derived from two words - (a) the Greek word “diabetes” meaning “siphon”, referring to the increased urination seen in this disease; and (b) the Latin word “mellitus” meaning “honey or sweet”, referring to the sweet taste of the urine caused by spilling out of excess sugar in the urine. Interestingly, there are two distinct disorders that share the first name “diabetes” - diabetes mellitus and diabetes insipidus. Both conditions are associated with excessive urine output and constant thirst. However, the hallmark of diabetes insipidus is the inability of the kidneys to conserve water, resulting in excretion of large quantities of dilute urine. It is important to note that individuals diagnosed with diabetes insipidus do not exhibit abnormal blood glucose levels.
Origin and Discovery of Diabetes
Diabetes is an old disease - ancient Egyptians documented clinical symptoms similar to those of diabetes mellitus in about 1500 BCE. Several ancient civilizations had recorded the fact that the urine of individuals with this condition had excess sugars (Ahmed, 2002). The condition was first called “diabetes” by the ancient Greek physician Aretaeus. “Mellitus” was later added to the name in 1675 by British physician and neuroanatomist Thomas Willis after rediscovering the sweet taste of urine and blood in patients. In 1889, German scientists Mering and Minkowski discovered the pancreatic origin of diabetes mellitus by showing that pancreactomy (removal of pancreas) in a dog could lead to diabetes-like symptoms. In 1910, Sir Edward Albert Sharpey-Schafer, founder of the field of endocrinology, discovered and named a hormone “insulin”, proposing that it was produced by the β-cells of the islets of Langerhans in the pancreas. In 1921 Frederick Banting and his medical student Charles Best showed that a protein extract from bovine pancreas containing insulin was able to lower blood glucose levels and effectively treat a pancreactomized dog. Soon thereafter they were able to apply this knowledge and treat terminally ill diabetic patients by injecting them with insulin.
Causes of Diabetes
Glucose is a key energy source for all cells in our body. It is derived directly from the food we eat (digestion and absorption), and is also supplied by the liver - either by breakdown of glycogen stores (glycogenolysis) or synthesis of glucose using other building blocks (gluconeogenesis). Insulin causes skeletal muscle and lipid cells in our body to take up glucose from the blood. Another hormone, glucagon, counters the insulin function and facilitates glucose production during periods of starvation.
Absence, inadequate supply, and improper function of insulin are some of the primary causes of diabetes. Causes of diabetes are also used to classify the types of diabetes. For example:
- Absence of insulin: Pancreatic cells producing insulin are selectively destroyed by an autoimmune response, leading to Type 1 diabetes
- Insulin Resistance: The individual may either have inadequate quantities of insulin in the body or problems with insulin function, both leading to Type 2 diabetes
- Inadequate insulin supply: Weight gain and obesity can lead to imbalance in the amount of insulin in relation to sensitivity of the cells to insulin
- Improper insulin function: Insulin binds to its receptor and initiates a cascade of signals in the cell, ultimately leading to the uptake of glucose. Missing or defective proteins in the signaling cascade (due to genetic defects or mutations) and/or changes in metabolites or signaling molecules (such as high levels of free fatty acids) may disturb the metabolic balance, leading to diabetes.
Although regulating glucose and insulin levels is central to managing diabetes, the roles of lipids and various stress-induced molecules in causing diabetes are being actively studied. Some of the key causes of diabetes are summarized in Figure 1. Note the impacts of physical inactivity, and weight gain.
Types of Diabetes
Most common types of diabetes, classified by causes and characteristics of the disease, are listed in Table 1 (“Diagnosis and classification of diabetes mellitus,” 2009). The hallmark for all forms of diabetes is high blood glucose levels. Assigning the type of diabetes mellitus is only important in understanding the pathogenesis in order to treat it effectively.
| Type | Causes/Characteristics | Clinical Profile/Comments |
| Type 1 Diabetes | Autoimmune; also knows as juvenile or insulin-dependent diabetes | Insulin is either not produced or produced in insufficient amounts due to β-cell destruction; requires supplemental insulin |
| Type 2 Diabetes | Polygenic; influenced by environment and lifestyle; also known as adult-onset or insulin-independent diabetes | Decreased responsiveness to insulin; increased incidence in individuals with obesity and family history of diabetes due to dual defects - insulin resistance and impaired insulin secretion capacity |
| Gestational Diabetes | Subset of Type 2 Diabetes; diagnosed as glucose intolerance during pregnancy | Insulin resistance; condition may persist after pregnancy |
| Prediabetes | May be genetic or environmental | May have arisen due to obesity and family history; usually can be mitigated by lifestyle changes |
| Maturity-onset diabetes of the young (MODY) | Monogenic; inherited in an autosomal dominant pattern; early age onset of hyperglycemia (generally before age of 25) | Impaired insulin secretion with minimal or no defects in insulin action |
| Secondary Diabetes | Induced by side effects of medications, infections, pancreas dysfunction (e.g. due to use of steroids, alcoholism, pancreatitis, etc.), or rare autoimmune disorders | Loss of pancreatic function, insulin resistance or impaired insulin secretion, depending on the specific cause(s) |
Symptoms
The main symptoms of diabetes are described as the three polys - polyuria, polydipsia, and polyphagia.
- Polyuria or the need to urinate frequently helps the body remove excess glucose that is filtered from the blood by the kidneys
- Polydipsia or increased thirst and fluid intake compensates for the loss of fluids resulting from increased urination
- Polyphagia or increased appetite compensates for the loss of glucose and fluids from the body, caused by excessive urination
Individuals with high risk for developing diabetes should be alert to these symptoms and seek medical attention if they notice the above symptoms.
Beyond the three "polys", other indicators for diabetes (listed by American Diabetes Association) include:
- Extreme fatigue
- Blurry vision
- Slow healing of cuts/bruises
- Weight loss
- Tingling, pain, or numbness in the hands/feet
In more advanced stages of diabetes, the following symptoms and diabetes complications may also be seen:
- Fainting and/or dizziness (possibly due to sudden drops in blood glucose levels due to poor management or increased medication)
- Foot ulcers (resulting from inability to attend to foot injuries due to loss of sensation in the extremities. These conditions may lead to gangrene and amputation)
- Peripheral neuropathy (loss of sensation, autonomic dysfunction)
- Retinopathy (blindness, blurred vision, or eye problems)
- Nephropathy (kidney damage)
- Damage to nerves (usually affects the extremities first) and bloods vessels, exposing diabetics to risk of cardiovascular complications (e.g., high blood pressure, heart disease, heart attack, stroke)
- Increased susceptibility to infections (e.g., urinary tract infections, sepsis, gangrene), since high glycemic environment provides a favorable medium for microbes
Risk Factors
Individuals may be susceptible to developing diabetes based on family history, age, ethnicity, and overall health. Therefore, clinicians recommend checking blood glucose levels in order to diagnose diabetes at early stages and prevent the complications associated with this disorder. Although the correlation between genetics and environmental factors with susceptibility to certain diabetes complications is not fully understood, maintaining good glycemic control remains a crucial mitigating factor in reducing rates of microvascular complications, cardiovascular events, and overall mortality.
Risks for developing Type 1 Diabetes: Recent exploration of human genomic regions associated with type 1 diabetes has identified candidate genes, gene products, and genetic loci that influence susceptibility to type 1 diabetes. Exposure to some viral infections (e.g., mumps), trauma (e.g., motor vehicle accident) and environmental factors (e.g., climate, and geographical location) could trigger the onset of type 1 diabetes. While gender does not appear to be a significant determinant of type 1 diabetes as incidence rates are generally similar for males and females, the risk of type 1 diabetes increases with age during childhood and adolescence (Dorman, 1997).
Risks for developing Type 2 Diabetes: People who are obese, have a family history of diabetes, or belong to high-risk ethnic groups (e.g., African American, Native American, Hispanic, and Pacific Islanders) should be regularly screened for the disorder. Environmental and behavioral risk factors, such as obesity and sedentary lifestyle, are also very important risk factors for developing this disease. Individuals of all ages diagnosed as prediabetic and pregnant mothers diagnosed with gestational diabetes are at high risk for developing type 2 diabetes.
Diagnosis
While symptoms may be indicative of disease, definitive diagnosis requires one or more of the following blood tests:
- Plasma glucose levels: The American Diabetes Association reports that the fasting plasma glucose (FPG) for normal individuals should be <100 126="" 140="" 2="" 8="" a="" after="" approximately="" as="" at="" be="" caloric="" defined="" diabetes="" diagnosis="" dl.="" dl="" fasting="" for="" glucose="" greater="" here="" hours="" implying="" intake="" is="" least="" less="" levels="" meal="" mg="" no="" occasions.="" of="" on="" overnight="" plasma="" requires="" should="" span="" than="" the="" two="" usually="">
Test Administration Risks Blood is drawn from the vein following overnight fasting (for fasting blood glucose levels) or at any random moment during the day (to measure random glucose levels). There may be some bruising, infection, and soreness at the site of puncture for drawing blood. The subject may also feel some dizziness.
- Oral Glucose Tolerance Test (OGTT) is an elaboration of the blood glucose test that reveals how the body metabolizes glucose ~2 hours after ingesting glucose. For pregnant mothers with high risk of diabetes, a glucose-screening test (OGTT) is usually performed between 24-28 weeks of pregnancy (or earlier) to identify gestational diabetes and manage the blood glucose levels for the health of mother and baby.
Test Administration Risks After blood is drawn, the subject is asked to drink a liquid, which contains 50, 75, or 100 grams of glucose. Normally the absorption of glucose in the body occurs rapidly, and blood glucose levels rise within 30 to 60 minutes of fluid intake. Blood work is done an hour after drinking the solution. If the blood test shows abnormal blood glucose levels, then blood work must be repeated after three hours. The blood test may cause side effects such as moderate pain, nausea, and faintness. Drinking the glucose solution may cause symptoms like shortness of breath, nausea, and vomiting, particularly in pregnant women with a predisposition to gestational diabetes mellitus.
- Hemoglobin A1c (or Hb A1c or A1c)refers to the percentage of glycated hemoglobin present in the blood. Prolonged exposure to high blood glucose levels leads to glucose attaching itself to proteins including hemoglobin. Since this happens over a period of time and is irreversible - the HbA1c test is not affected by random fluctuations due to temporary alteration in diet, lifestyle, stress or illness of the subject. Maintaining an HbA1c below 5.7% is indicative of normal health. An HbA1c level of 5.7-6.4% signals prediabetes, and any values higher than 6.4% indicates a diabetic condition requiring treatment.
Test Administration Risks A sample of blood is taken either from a finger stick or by drawing a small vial of blood from a vein (venipuncture) and is tested. Obtaining a blood sample for the test may lead to light-headedness or fainting of the subject. It may also lead to infection, excessive bleeding, or hematoma (localized abnormal accumulation of blood under the skin) at the site of puncture for drawing blood.

Complications
Uncontrolled diabetes can cause metabolic imbalance leading to acute complications that may require immediate medical attention. Hyperglycemia (high levels of glucose in blood) sets the stage for protein glycation, which in turn may lead to chronic conditions requiring constant monitoring and treatment. Individuals with diabetes may also develop high cholesterol and high blood pressure, which require medical management.
Acute Complications - Require Immediate Medical Intervention
- Ketoacidosis: Despite high blood glucose levels, the body cells (muscle and lipid cells) may be starved for glucose due to absence or improper function of insulin. Cells may also starve for glucose if the amount of food intake is low (such as during illness) or if the dosage of insulin is too high. Under these conditions cells start using fats as a source of energy. Liver cells produce ketone bodies from fatty acids. When the glucose levels are low, brain cells can use ketone bodies, but not free fatty acids, for energy. High concentrations of ketones can make the urine acidic and cause fruity-smelling breath. If not managed, this condition can progress to coma (prolonged unconsciousness) and even death.
- Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS): High blood glucose level triggers increased urination. If liquids are not replaced, the individual can become severely dehydrated. High blood glucose levels can lead to altered mental states, confusion, seizures, coma, and even death.
Chronic Complications - Long-term Side Effects of Diabetes
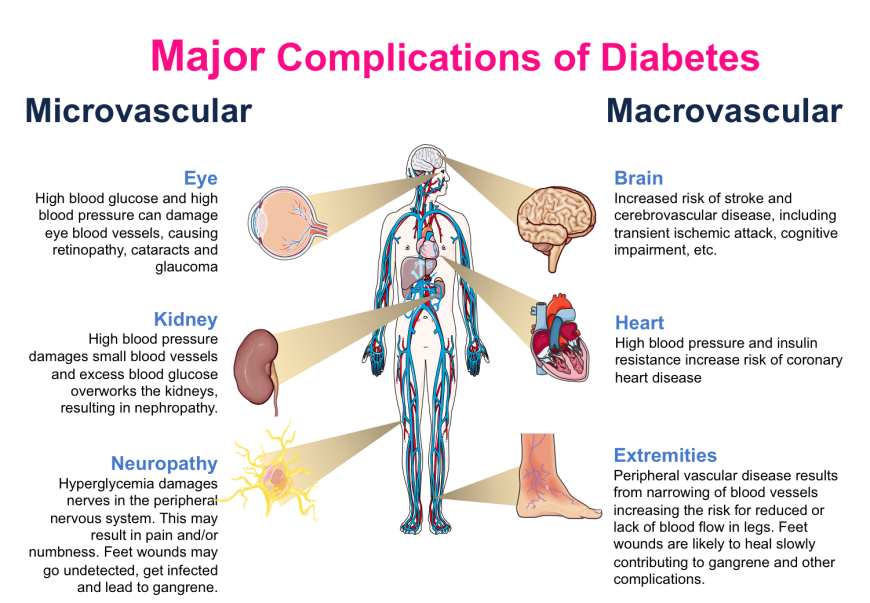
- Microvascular complications affect the smaller blood vessels, such as in the eyes (leading to retinopathy), kidneys (leading to nephropathy), and neurons (leading to neuropathy). Individuals with poorly managed blood glucose levels may suffer from one or more of these complications in advanced stages of the disease. Thus, besides monitoring the health of eyes and kidneys, diabetics also require foot care. Interestingly, several large population studies have shown that aggressive management of blood glucose levels (i.e., keeping blood glucose levels within a narrow range) can avoid, or at least delay, the onset of these complications (Nathan et al., 2014). Regular monitoring and management of blood glucose levels is of critical importance in maintaining metabolic balance and avoiding microvascular complications.
- Macrovascular complications affect larger blood vessels, such as those supplying the heart, brain, and extremities. The causes of these complications stem from narrowing of blood vessels due to glycation, inflammation, lipid deposition and other factors. Complications resulting from large vessel damage may lead to cardiomyopathy, stroke, rheumatoid arthritis, osteoporosis, and the degenerative process of aging (Singh et al., 2014). The major concern amongst these complications is myocardial infarction (heart attack). At present, it appears that blood glucose control does not significantly reduce the risks or delay the onset of macrovascular complications. Additional medical management is required.
Non-Pharmacological
The cornerstone of diabetes management is tight glycemic control. The first line of action upon noticing any symptoms of type 2 diabetes should be lifestyle changes, i.e., managing blood glucose levels by regulating diet (both quality and quantity of nutritional intake) and exercise. Through these changes, individuals diagnosed as prediabetic can often check their progression to full-blown disease. Individuals diagnosed with diabetes, who are taking medications can also benefit from these lifestyle changes.
Diet: High blood sugar levels can be managed by reducing caloric intake, either by careful portion control or by choosing foods that have lower glycemic loads. Foods made from refined sugars and easily digestible starches, such as white bread, sugary drinks, etc., lead to sudden increases (spikes) in blood glucose levels and are likely to promote metabolic imbalances. On the other hand, foods rich in fiber, such as whole grains, fruits, and vegetables take time to be digested, do not prompt rapid rise in blood glucose levels, and favor metabolic balance.
Exercise: Exercise has many health benefits, the most obvious of which may be improved glucose homeostasis and insulin sensitivity. Exercise stimulates skeletal muscles to take up more glucose from the blood. In addition, it reduces the amount of lipids stored in fat cells, while also making them more sensitive to insulin action.
Glucose Homeostasis:
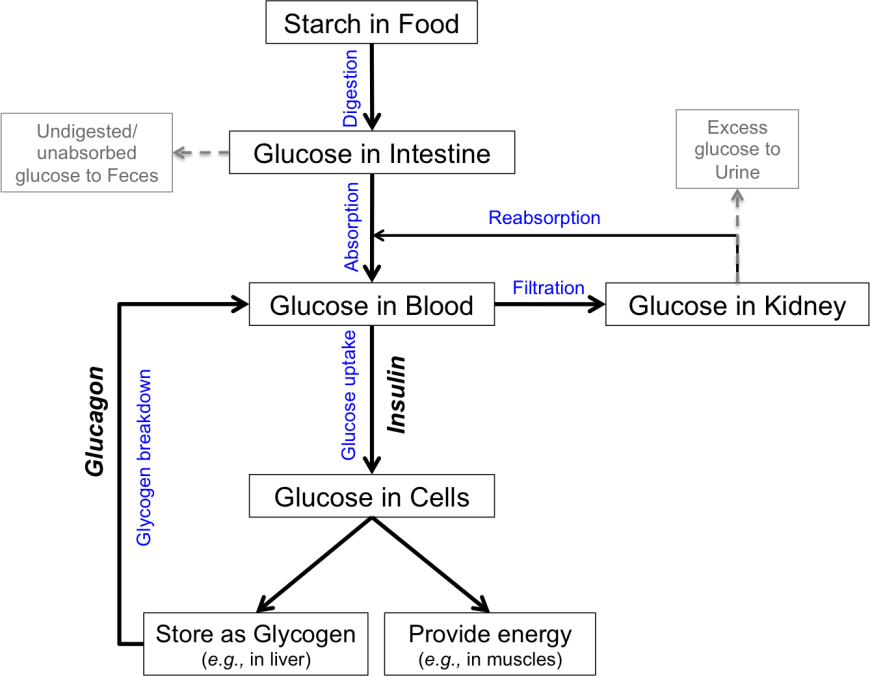
The food that we eat is our main source of glucose. Starches and sugars in our food are digested and glucose is absorbed into the blood (Figure 1). Some cells in the body, such as brain cells, can take up glucose without insulin, via specific glucose transporters (GLUT 3). Most other cells, such as muscle and lipid cells, require insulin function in order to take in glucose from the blood. Once in the cell, glucose is either used for energy or stored (for example, as glycogen in liver). During periods of starvation, the hormone glucagon triggers conversion of glycogen back to glucose. When kidneys filter the blood, any unused glucose enters the filtrate. If needed, this glucose can be reabsorbed, while excessive amounts of glucose in the filtrate can be eliminated in the urine. Figure 1 shows an insulin centric view, where the presence of insulin is critical to glucose uptake by cells.
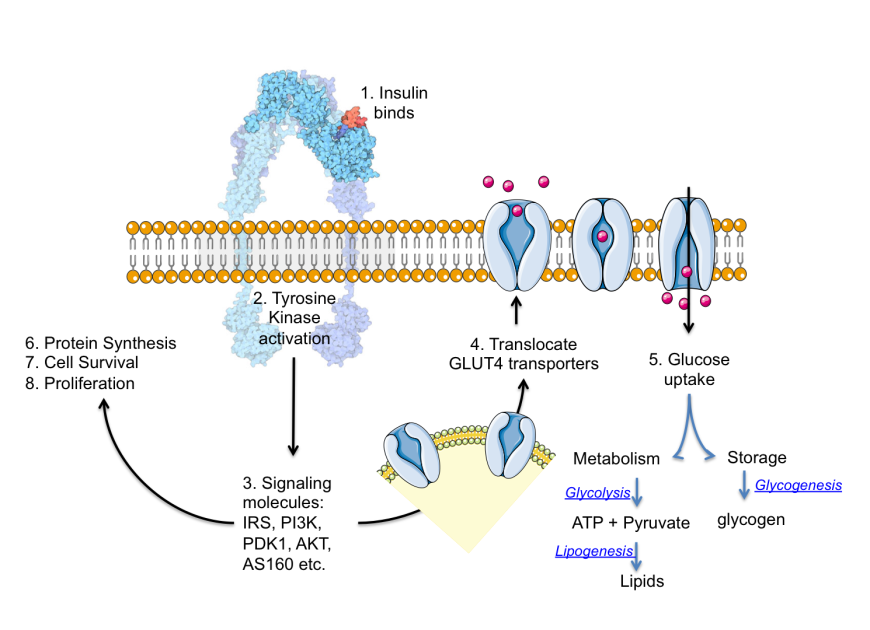
Insulin binds to cell surface receptors to initiate a signaling cascade (Figure 2) that in turn mobilizes glucose transporter proteins to the cell surface to take up glucose. In the absence of the insulin generated signals, these transporter proteins are sequestered in the cell so the cells cannot take up glucose. Exercise activates other signals that can also translocate GLUT4 transporters to the cell surface. This is one of the mechanisms by which exercise increases insulin sensitivity.
Pharmacological
The main objective for treatments of diabetes is prevention of hyperglycemia and reduction of protein glycation to avert complications. The success of treatment is commonly monitored via Hb A1c levels. Furthermore, since diabetes may greatly increase risk for cardiovascular diseases, it is essential to control blood pressure and cholesterol levels as part of the treatment regimen. Here, we mainly discuss the pharmacological treatment options for managing blood glucose levels. The strategies discussed include altering specific functions in glucose homeostasis using small molecule drugs and/or including specific hormones and/or its analogs to enhance their levels and functions.
Treating type 1 diabetes: The treatment for type 1 diabetes is administration of insulin via injection or pump (see Insulin in Figure 1). Short-acting and long-acting insulins are typically used in combination. Long-acting insulins direct a basal level of sugar uptake by cells throughout the day, while short-acting insulins cover glucose level increases following meals. Learn more about designer insulins here.
Treating type 2 diabetes: There are various classes of non-insulin anti-diabetes medications that are used to treat type 2 diabetes. Here we discuss five main strategies for managing blood glucose levels (see Figure 1):
- Increasing insulin secretion may be accomplished by various classes of drugs. Some drugs increase release of insulin stored within the pancreatic β-cells, while other drugs promote insulin production and release.
- Increasing insulin function can enhance glucose uptake and utilization thereby facilitating lowering of blood glucose.
- Decreasing glucose production from liver stores of glycogen can reduce elevated blood glucose levels after overnight fasting.
- Decreasing glucose absorption from the food can be accomplished by blocking the breakdown of starch into glucose. Undigested starch is excreted in feces.
- Decreasing glucose reabsorption from the kidneys reduces blood glucose levels. Excess glucose is eliminated in urine.
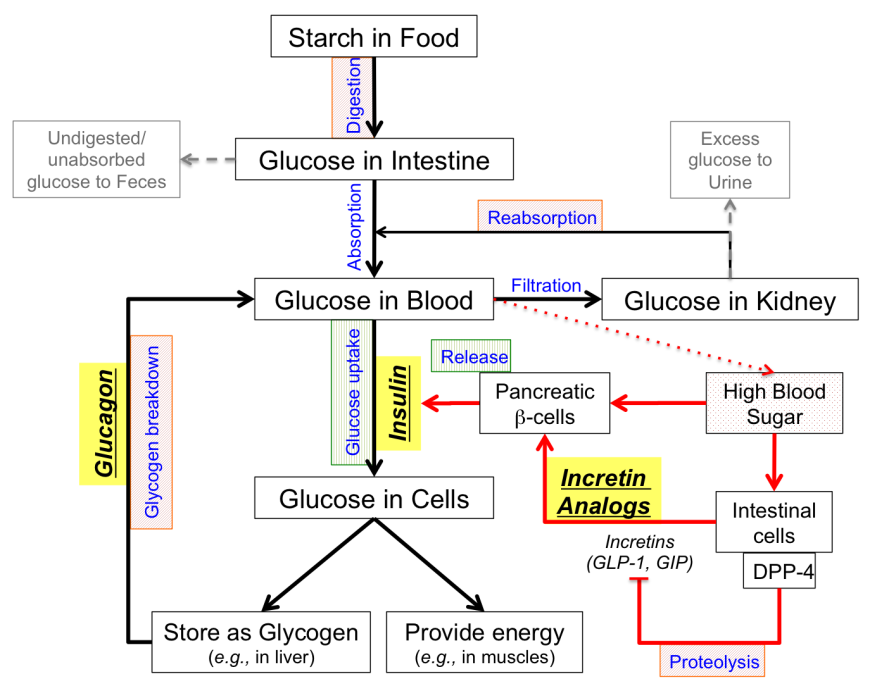
Figure 1: Glucose homeostasis concept map showing strategies for treating type 2 Diabetes. The red arrows indicate how an individual would respond to high blood sugar. Processes targeted for treatment are colored and shaded - processes in green boxes (vertical line shading) are increased in treatment, while processes in red boxes (diagonal line shading) are decreased for treatment. Exogenous hormone analogs used for treatment are shown in bold italics and highlighted in yellow colored boxes.
How does the doctor decide which drug(s) to prescribe?
If the individual has type 1 diabetes, the only approved treatment is insulin administration.
Treatment plans for type 2 diabetes have various options and require careful decision. Immediately after a pre-diabetes diagnosis, the first line of action should be to make lifestyle changes to restrict calories, eat healthier, and exercise more to reduce weight and become active. If these measures fail to manage high blood glucose levels, the first drug commonly prescribed for treating type 2 diabetes is Metformin. The strategy here is to reduce glucose production by the liver and increase insulin sensitivity. If increasing dosage of this drug does not work (or if the individual has renal disease), Sulfonylureas (such as Glipizide) may be added to increase insulin secretion. Other classes of drugs (such as incretins or DPP4 inhibitors or Meglitinides) may also be used to achieve the same result - increased insulin secretion. When increased endogenous insulin fails to manage high blood glucose, the individual probably has severe insulin resistance, and drugs that increase insulin sensitivity (such as Thiazolidinediones) are often prescribed. At this stage, the doctor may also resort to alternative approaches to reducing the blood sugar load (e.g., alpha glucosidase inhibitors can reduce the amount of glucose absorbed from food or SGLT-2 inhibitors can reduce the reabsorption of glucose from kidneys so that the excess sugar is eliminated in urine). Finally, if all these approaches fail, the doctor may resort to adding insulin or completely switching to insulin for blood glucose management.
Ideally, diabetes treatment plans should be reviewed every 3-4 months to evaluate whether the prescribed drug(s) are adequate to manage the individual's diabetes. Many factors such as medication costs, access to medications, ability to tolerate the side-effects, and other medical conditions, may play critical roles in deciding the individual's treatment plans.
Less
Classes of drugs used to treat individuals with diabetes mellitus (specifically type 2 diabetes) are summarized in the table below. Each class of drug uses a different strategy to lower blood glucose. Their targets and mechanisms of action are also summarized:
| Enhancers of insulin secretion by β-cells | |
Sulfonylureas
Role(s): Enhances insulin secretion by pancreatic β-cells.
Target(s): ATP-binding cassette sub-family C member 8
Mechanism of Action: Binds to ligand-specific receptor on cytoplasmic face of pancreatic β-cells, mediating closure of ATP-sensitive K+ channel, causing depolarization, and calcium entry into cell, thereby stimulating insulin release.
Administration: Take with meals once or twice a day.
Possible side effects: Hypoglycemia.
US FDA approved drugs: Chlorpropamide (Diabinese), Glimepiride (Amaryl), Glipizide (Glucotrol), Glyburide (DiaBeta), Tolazamide (Tolinase), Tolbutamide (Orinase)
| 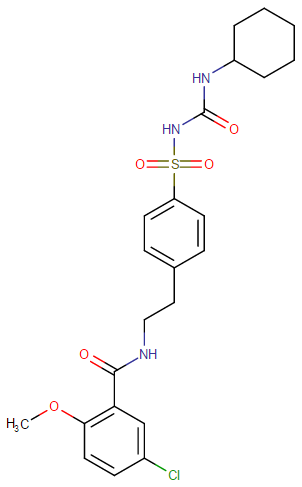
Representative Chemical Structure: Glyburide (DrugBank)
|
Meglitinides
Role(s): Enhances insulin secretion by pancreatic β-cells.
Target(s): ATP-binding cassette sub-family C member 8
Mechanism of Action: Binds to ligand-specific receptor on cytoplasmic face of pancreatic β-cells, mediating closure of ATP-sensitive K+ channel, causing depolarization, and calcium entry into cell, thereby stimulating insulin release.
Administration: Take before meals.
Possible side effects: Hypoglycemia
US FDA approved drugs: Repaglinide (Prandin), Nateglinide (Starlix)
N.B.: Meglitinides are designed to avoid hypoglycemia that may result as a side of effect of sulfonylurea administration. In comparison to sulfonylureas, they have shorter half-live and are taken at mealtimes to enhance insulin secretion and prevent postprandial (i.e., occurring after a meal) hyperglycemia.
| 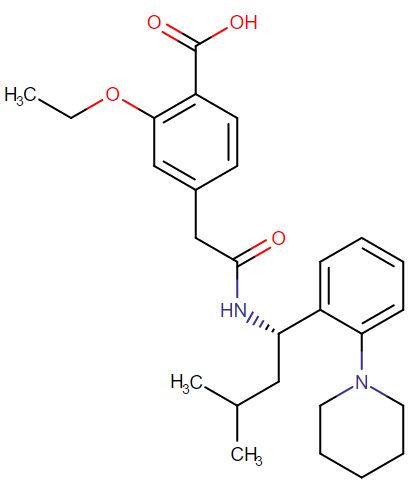
Representative Chemical Structure: Repaglinide (DrugBank)
|
Glucagon-Like Peptide-1 Analogs – peptide drugs with a longer half-life than the natural GLP-1 hormone, because they are resistant to degradation by the enzyme dipeptidyl peptidase 4 (DPP-4).
Role(s): Enhances insulin secretion by pancreatic β-cells.
Target(s): Glucagon-Like Peptide-1 receptor
Mechanism of Action: Binds to the GLP-1 receptor and stimulates insulin secretion from the pancreatic β-cells; inhibits glucagon secretion and function; delays gastric emptying into the small intestine, signals satiety and thereby suppresses food intake.
Administration: Inject peptide daily; now longer acting versions (once a week injections) are also available.
Possible side effects: May cause nausea and eventually lead to pancreatitis.
US FDA approved drugs: Liraglutide (Victoza), Exenatide (Bydureon) (injected)
| 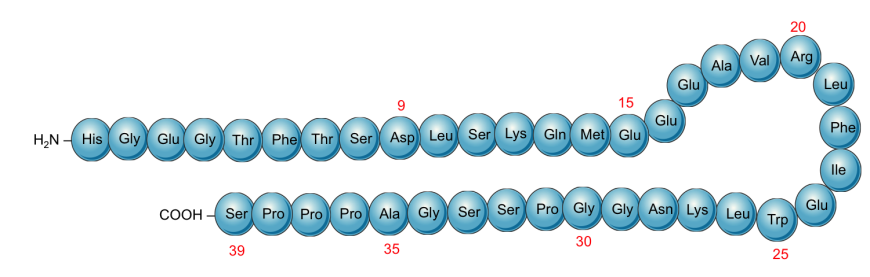
Schematic representation of the primary structure of Exenatide showing the sequence of the protein (derived from Gila monsters)
|
Dipeptidyl Peptidase-4 Inhibitors
Role(s): Enhances insulin secretion by pancreatic β-cells indirectly by prolonging the half-life or action of endogenous GLP-1.
Target(s): Dipeptidyl Peptidase-4
Mechanism of Action: Inhibits the enzyme DPP-4, resulting in increased activity of incretins (e.g., GLP-1); leads to increased insulin secretion, decreased gastric emptying, and thus lowers blood glucose levels.
Administration: Take orally once a day (at the same time each day).
Possible side effects: May lead to pancreatitis.
US FDA approved drugs: Sitagliptin (Januvia), Linagliptin (Tradjenta), Saxagliptin (Onglyza), Alogliptin (Nesina), Vildagliptin (Galvus), Anagliptin (Suiny, Beskoa), Omarigliptin (Marizev – Merck has suspended development and marketing of omarigliptin)
| 
Representative Chemical Structure: Sitagliptin (DrugBank)
|
| Suppressors of Endogenous Glucose Production | |
Biguanides
Role(s): Suppresses hepatic gluconeogenesis and enhances insulin action in muscle/fat.
Target(s): 5’AMP-activated protein kinase subunit β-1
Mechanism of Action: Inhibits glucose production by the liver; increases insulin sensitivity, and stimulates glucose uptake in tissues; does not stimulate the pancreas to manufacture or secrete more insulin.
Administration: Take orally twice a day with meals.
Possible side effects: May cause gastrointestinal complications (e.g., nausea, vomiting) and risk of lactic acidosis, especially in the elderly and in those with compromised kidney function.
US FDA approved drugs: Metformin (Glucophage). Also approved in fixed dose combinations with antidiabetic drugs from other classes.
| 
Representative Chemical Structure: Metformin, the first line biguanide
|
Amylin Agonists – Synthetic analogs of the 37 amino acid peptide, amylin (islet amyloid polypeptide or IAPP), which is cosecreted with insulin by pancreatic β-cells and is synergistic in function in maintaining glycemic control.
Role(s): Suppresses hepatic gluconeogenesis.
Target(s): Amylin receptor
Mechanism of Action: Inhibits glucagon secretion and lowers preprandial rise in glucose levels; delays gastric emptying, promoting satiety, and thus inhibiting food intake.
Administration: Subcutaneous injection.
Possible side effects: Gastrointestinal complications (nausea, vomiting, abdominal pain), headache, dizziness, anorexia, fatigue and coughing.
US FDA approved drugs: Symlin (pramlintide)
N.B.: This is typically used in adjunction to insulin or metformin.
| 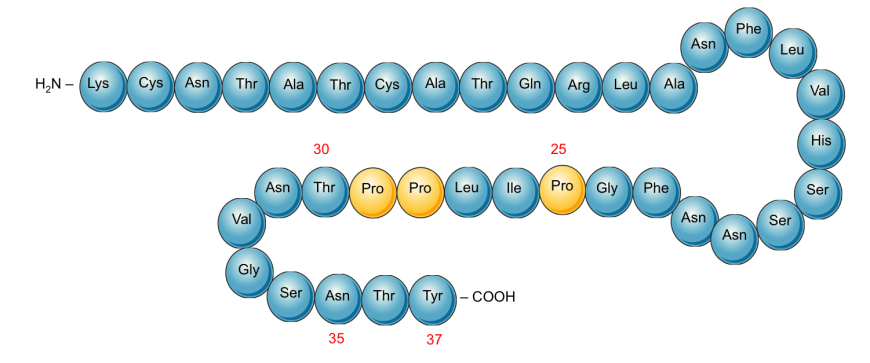
Schematic representation of the primary structure of Pramlintide. Proline substitution (changed compared to the native Amylin) at positions 25, 28, and 29 (highlighted in yellow) prevents aggregation and amyloid formation.
|
| Enhancers of insulin action in the periphery | |
Thiazolidinediones (TZDs)
Role(s): Enhances insulin sensitivity in muscle/fat cells, addressing a key problem in type 2 diabetes (i.e. insulin resistance). It also suppresses hepatic gluconeogenesis (i.e. glucose production from lipids and protein components).
Target(s): Peroxisome proliferator-activated receptor gamma (PPAR-γ)
Mechanism of Action: Acts as agonist of PPAR-γ, lowers insulin resistance and increases glucose uptake by muscle cells.
Administration: Take orally once a day at the same time.
Possible side effects: Slow onset of action, may increase risk of cardiovascular problems, fluid retention, accumulation of adipose tissue, bone loss.
US FDA approved drugs: Rosiglitazone (Avandia), Pioglitazone (Actos)
| 
Representative Chemical Structure: Rosiglitazone (DrugBank)
|
| Blockers of GI tract carbohydrate absorption | |
Alpha-glucosidase Inhibitors
Role(s): Inhibits breakdown of starches in gastrointestinal tract, indirectly reducing absorption of dietary carbohydrates.
Target(s): α-glucosidase enzymes in gut
Mechanism of Action: Works by competitively and reversibly inhibiting α-glucosidase (an enzyme responsible for degrading carbohydrates), thus slowing digestion of carbohydrates and delaying glucose absorption.
Administration: Take with first bite of meal.
Possible side effects: Gastrointestinal complications (nausea, vomiting, diarrhea).
US FDA approved drugs: Acarbose (Precose), Miglitol (Glyset: oral, not absorbed)
| 
Representative Chemical Structure: Acarbose (DrugBank)
|
| Blockers of glucose reuptake in the kidney | |
Sodium-glucose transport-2 (SGLT-2) Inhibitors
Role(s): Block reabsorption of glucose from urinary tract.
Target(s): Na+/Glucose Cotransporter 2 in kidney.
Mechanism of Action: Reduces renal glucose reuptake, resulting in an increased amount of glucose excreted in urine.
Administration: Take orally once a day.
Possible side effects: Polyuria, urinary tract infections, dehydration, ketoacidosis.
US FDA approved drugs: Canagliflozin (Invokana), Dapagliflozin (Farxiga), Empagliflozin (Jardiance)
| |












0 Comments